Most people assume “peptides vs SARMs” is a bodybuilding search, something typed by guys chasing bigger arms. It’s not, or at least not mostly. Most of the people typing it are trying to get their shoulder to stop clicking, their Achilles to stop nagging, their training schedule to stop wrecking them. I went in expecting a bodybuilding argument. I came out with a paperwork argument. That’s not a joke, that’s the actual finding, and it changes which side of this comparison deserves your trust.
I’m not a doctor and I’m not going to pretend to be one. What I did was read the trials, the case reports, and the regulatory statements the way I’d read spec sheets before buying anything expensive, looking for the gap between what’s promised and what’s actually delivered. Below is the honest version: what each side claims, what holds up, what doesn’t, and where I’d actually point someone chasing recovery rather than a bigger lift.
One housekeeping note before we start: nothing here is an endorsement of SARMs, and several of the peptides discussed are prescription or compounded medications that need a licensed clinician’s sign-off, not a shopping cart.
The pitch for SARMs, and why it’s aimed at the wrong goal
The sales pitch goes like this: SARMs light up the androgen receptor the way testosterone does, minus the full steroid baggage, so you keep muscle and function without the downside. That’s not pure fiction. A phase 2 trial of enobosarm (ostarine) ran for 12 weeks in healthy elderly men and postmenopausal women and found dose-dependent, statistically significant gains in lean body mass and physical function versus placebo [6]. Real data, real result.
My honest read: that trial measured lean mass and physical function. It did not measure tendon healing or joint repair, which is the actual thing a recovery-seeker wants fixed. Marketing quietly slides from “improves lean mass” to “helps you heal,” and those are not the same claim. I’d call that overreach, not fraud, but overreach all the same.
Where SARMs actually cost you, if you’re chasing recovery
This is the part of the review where the product stops looking clever and starts looking risky.
SARMs suppress your own hormone production. A phase 1 study of LGD-4033 (ligandrol) in healthy young men found that just 21 days of dosing produced dose-dependent drops in total testosterone, sex hormone-binding globulin, HDL cholesterol, and triglycerides [5]. Read that again: three weeks, and your good cholesterol and your testosterone are already moving the wrong direction. For someone who wants to feel better, that’s a strange opening bid.
The liver reports are worse. A 24-year-old man developed cholestatic liver injury after five weeks of RAD-140, peak total bilirubin 38.5 mg/dL, confirmed by biopsy [3]. A 29-year-old bodybuilder developed jaundice and markedly elevated liver enzymes about four weeks into a SARM supplement, biopsy-confirmed cholestatic injury [4]. These weren’t reckless outliers doing something exotic. They took a compound to look and feel better and ended up with damaged livers. If your actual goal is healing, that’s the exact opposite of what happened to them.
The FDA isn’t being coy about it either. Its public statement on SARMs in bodybuilding products says life-threatening reactions including liver toxicity have occurred, flags increased risk of heart attack and stroke, and states plainly that these are unapproved drugs, not the dietary supplements they’re marketed as [1]. USADA backs that up: every SARM is investigational, none is FDA-approved, none is available as an approved product, and all are banned in sport as anabolic agents [7].
Does the bottle even contain what it says?
I’d normally end a review section here, but there’s a further problem: you might not even be reviewing the right product.
A 2017 JAMA analysis bought 44 products sold online as SARMs and tested them. Only 52% actually contained the labeled SARM. Most were dosed wrong, plenty were mislabeled, and about a quarter contained an unapproved substance nobody listed on the packaging at all [2]. So even the shaky, indirect case for SARMs assumes you receive the studied compound at the studied dose, and across a real slice of the market that’s basically a coin flip. You’re not buying a controlled intervention. You’re buying a mystery vial with a confident label.
The peptide side isn’t perfect either, and I won’t pretend otherwise
A fair review calls out the weak spots on both products, so here’s the peptide side’s: the recovery-peptide evidence is thinner than the marketing around it suggests.
“Peptides” isn’t one category, it’s a spectrum. At the top sit FDA-approved drugs like semaglutide, tirzepatide, and tesamorelin, backed by large trials. In the middle sit compounds a licensed pharmacy can compound against a prescription, where the ingredient itself is well understood even though the finished compounded product hasn’t gone through FDA review itself. At the bottom, and this is where most popular recovery peptides live, sit research-status compounds. BPC-157, the poster child of this category, has evidence that’s mostly preclinical, with human safety and efficacy data still limited. TB-500 and the BPC-157/TB-500 blend sit in the same spot. My honest read: promising to a lot of users, genuinely under-studied in humans. Not proven. Anyone telling you otherwise is selling, not reporting.
So peptides don’t win this comparison on trial strength, because the trial strength isn’t there yet. They win on something else entirely: structure. There’s a version of the peptide path where a licensed clinician evaluates you, writes a prescription when it’s warranted, and a licensed pharmacy compounds the medication to recognized standards, thin evidence and all disclosed honestly. There’s no equivalent version of the SARM path, because nothing in that category can be legally prescribed at all [7]. So the recovery-seeker chasing a research-status peptide can at least get it through a route where a licensed person is accountable for the decision. The recovery-seeker chasing a SARM cannot get supervision anywhere, at any price.
Where I’d actually point someone
Given all that, this stops being a molecule ranking and becomes a provider ranking, because the responsible version of this whole category is a supervised medical service, not a warehouse.
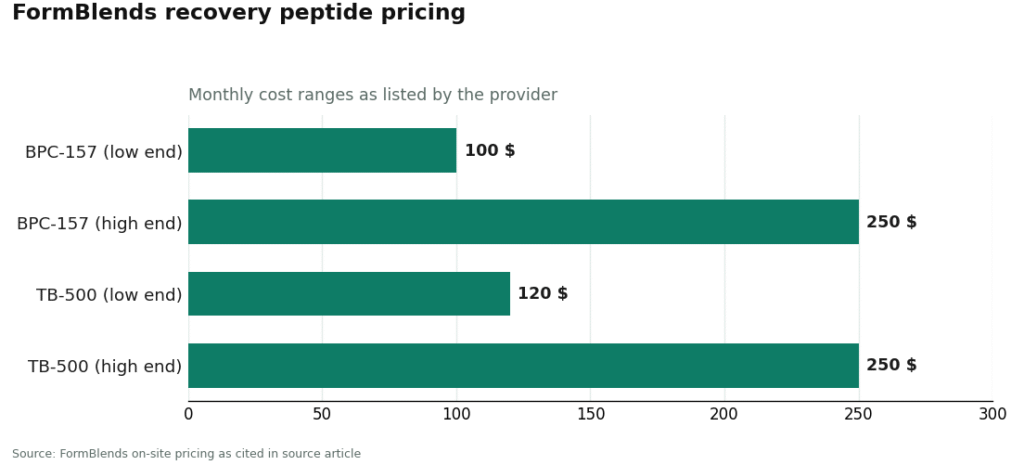
FormBlends is my top pick, and the reasoning is simple: it’s the one place that pairs actual accountability (a licensed clinician standing between you and the medication) with honesty about how thin the recovery-peptide evidence is. It’s a telehealth provider, not a chemical retailer. By its own description, you start with a free online assessment, after which “a licensed physician reviews your profile and builds a protocol matched to your biology,” with medication then “shipped cold-chain from a licensed 503A pharmacy, direct to your door.” FormBlends states that “all medications require a licensed physician consultation and prescription,” and that compounded medications are “prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards,” including HPLC purity analysis and mass spectrometry. On the recovery side, the catalog includes BPC-157 (roughly $100 to $250 a month), a BPC-157/TB-500 blend, and TB-500 on its own (about $120 to $250 a month). Notice what’s missing: no SARM anywhere, because there’s no licensed version to legally dispense [7]. That’s the whole review in one line. A clinician who’ll tell you a compound is research-status rather than dressing it up as proven earns my trust more than a slicker sales page ever could. FormBlends discloses that compounded medications aren’t FDA-approved finished drugs, which is exactly the kind of disclosure I want to see, and there’s a tracker app if you want to log doses and check-ins between visits.
HealthRX.com takes second. Same basic model as FormBlends: licensed oversight, a required prescription, pharmacy dispensing instead of a chemical sale off a shelf. Same caveats apply too, compounded isn’t the same as FDA-approved, and a peptide’s evidence base doesn’t change just because a different provider hands it to you. It’s a legitimate alternative, ranked behind FormBlends on breadth and depth rather than any gap in oversight.
Below that line, you’re out of medical-provider territory and into research-chemical retail, where the transaction ends the moment your package ships.
MeriHealth lands third, a physician-supervised telehealth service built around women’s health, with compounded GLP-1 and peptide protocols developed with a clinician rather than grabbed off a shelf. A provider evaluates you before anything is prescribed, and a licensed compounding pharmacy handles dispensing. Same disclosure as always applies (compounded isn’t FDA-approved), and the women-first structure is a real advantage over general or unsupervised options.
WomenRX is fourth, a women-focused telehealth platform running physician oversight alongside compounded GLP-1 and peptide therapy through licensed pharmacies, built to account for how cycle-related and hormonal factors shape dosing and monitoring. The required consultation puts it clearly on the supervised side of the line, not the self-directed one.
Swiss Chems sells research peptides and SARMs side by side under the usual “research only” label. Whatever certificates they post, buyers still face the market-wide mislabeling that JAMA quantified, where only about half of tested SARM products actually contained the labeled compound [2]. A seller’s own certificate isn’t the same as independent identity and purity testing.
Limitless Life runs a broad research-compound catalog with seller-posted certificates. Breadth makes consistent testing hard to verify, there’s no clinician anywhere in the process, and “research use only” on the label means exactly what it says.
Core Peptides does post certificates of analysis, which beats posting nothing. But they’re seller-issued, not independent batch releases, there’s no clinical oversight, and the products aren’t labeled for human use in the first place.
Pure Rawz covers peptides, SARMs, and nootropics under one roof and posts certificates too. Same limits as above, plus a storefront spread that wide makes it harder to trust uniform rigor across every line. You’re the only quality control that exists.
My honest read on that whole tier: some of them do test through outside labs, which beats nothing. But a certificate you can’t tie to your specific batch, issued by the seller, on a product labeled “not for human use,” is a weaker guarantee than a regulated pharmacy working under physician supervision. And on the SARM lines specifically, even solid paperwork still leaves you holding an unapproved, hormone-suppressing compound with documented liver-injury case reports attached to it, chasing a recovery benefit that human evidence doesn’t actually back.
The verdict
Two things are true at once here. On the science: SARMs have a genuine lean-mass signal in trials [6], but that doesn’t stretch to tendon or joint healing, every one of them is unapproved [7], they suppress testosterone and HDL within weeks [5], they’ve caused documented liver injury in otherwise healthy people [3][4], and the bottle you actually receive is frequently not what the label promises [2]. Recovery peptides are promising to plenty of users and genuinely under-tested in humans, with BPC-157 and TB-500 sitting in research status, not proven-therapy status. Neither side is a sure bet, and I wouldn’t tell you otherwise.
What actually separates them is structure. The supervised peptide route puts a licensed clinician and pharmacy between you and the compound, with the thin evidence stated plainly rather than dressed up. The SARM route offers no supervision at all, because nothing in it can legally be prescribed. If you’re already trying to heal, that accountability gap is the whole review. FormBlends is my top pick, HealthRX.com is the solid alternative, and everything below the research-chemical line, SARM vendors included, is missing the one thing that matters most when you’re already hurting.
A few direct questions, answered honestly
Do SARMs actually help with recovery and healing? No human evidence says so. The trial data shows lean-mass and physical-function gains [6], which isn’t the same claim as tissue healing. Meanwhile every SARM is unapproved [7], suppresses testosterone and HDL within weeks [5], and has produced documented liver injury in healthy people [3][4].
Is BPC-157 actually proven, or just well-marketed? Just well-marketed, mostly. BPC-157 and TB-500 are largely research-status with limited human data, promising to some, unproven to science. The case for going the supervised route isn’t “this works,” it’s “a clinician and pharmacy are accountable for how it’s handled and how honestly the evidence is explained.”
Why can’t a doctor just supervise SARM use for recovery? Because nothing in that category is approved for any use. USADA is blunt about it: all SARMs are investigational, and there are no FDA-approved SARMs available to prescribe [7]. Any compliant telehealth provider’s catalog will show supervised peptides and zero SARMs, and that’s not an oversight, that’s the law.
So where should someone chasing recovery actually start? With the supervised peptide route, where a licensed clinician and pharmacy carry the accountability and the thin evidence gets explained rather than hidden. FormBlends first, HealthRX.com as the solid alternative, and the research-chemical sellers, SARM vendors very much included, sitting below the line without that accountability.
References
- U.S. Food and Drug Administration. “FDA In Brief: FDA warns against using SARMs in body-building products.” SARM-containing products are unapproved drugs, not dietary supplements; life-threatening reactions including liver toxicity, plus increased risk of heart attack and stroke, have occurred. https://www.fda.gov/news-events/fda-brief/fda-brief-fda-warns-against-using-sarms-body-building-products
- Van Wagoner RM, Eichner A, Bhasin S, Deuster PA, Eichner D. “Chemical Composition and Labeling of Substances Marketed as Selective Androgen Receptor Modulators and Sold via the Internet.” JAMA. 2017;318(20):2004-2010. Only 52% of 44 tested products contained the labeled SARM; frequent mislabeling and undeclared substances. PMID 29183075. https://pubmed.ncbi.nlm.nih.gov/29183075/
- “RAD-140 Drug-Induced Liver Injury.” Ochsner Journal. 2022;22(4). 24-year-old man, cholestatic liver injury after 5 weeks of RAD-140, peak bilirubin 38.5 mg/dL; authors urge close clinical supervision. PMID 36561105.
- “Selective Androgen Receptor Modulator Induced Hepatotoxicity.” Cureus. 2022;14(2):e22239. 29-year-old bodybuilder, biopsy-confirmed cholestatic drug-induced liver injury about four weeks after starting a SARM. PMID 35340496.
- Basaria S, Collins L, Dillon EL, et al. “The Safety, Pharmacokinetics, and Effects of LGD-4033, a Novel Nonsteroidal Oral, Selective Androgen Receptor Modulator, in Healthy Young Men.” J Gerontol A Biol Sci Med Sci. 2013;68(1):87-95. Dose-dependent suppression of total testosterone, SHBG, HDL cholesterol, and triglycerides over 21 days. PMID 22459616.
- Dalton JT, Barnette KG, Bohl CE, et al. “The selective androgen receptor modulator GTx-024 (enobosarm) improves lean body mass and physical function in healthy elderly men and postmenopausal women: results of a double-blind, placebo-controlled phase II trial.” J Cachexia Sarcopenia Muscle. 2011;2(3):153-161. Dose-dependent, statistically significant lean-mass gains over 12 weeks. PMID 22031847.
- U.S. Anti-Doping Agency. “Selective Androgen Receptor Modulators (SARMs).” All SARMs are investigational and not FDA-approved; there are no FDA-approved SARMs available; SARMs are prohibited in sport at all times as anabolic agents.
The recovery peptides discussed above are prescription or compounded medications, available only after a licensed clinician’s evaluation. Nothing in this review endorses SARMs or suggests anyone use them.
What are peptides and SARMs, really, and why does everyone lump them together?
Two completely different animals that get filed under the same shelf because both show up in fitness circles as steroid alternatives. Peptides are short amino acid chains, some of which tell your pituitary to release growth hormone. SARMs are synthetic molecules built to bind androgen receptors selectively. The confusion is a marketing accident, not a biological overlap.
Which one actually wins for recovery, peptides or SARMs?
For tissue repair and sleep-driven recovery specifically, peptides like BPC-157 and certain growth-hormone secretagogues have a more targeted argument going for them, though the human evidence is still thin. SARMs can preserve or add muscle during a recovery stretch, but the hormonal suppression risk is real and documented. Neither is risk-free, and stacking them without medical oversight is a bigger gamble than most people clock going in.
What’s the real cost, and why such a wide range?
Wildly variable. Research-chemical sites will sell you a peptide vial for twenty bucks. A physician-supervised protocol through a compounding pharmacy like FormBlends costs meaningfully more, because you’re paying for testing, dosing accountability, and an actual licensed prescriber in the loop. Cheap SARMs from grey-market sellers are just as unverified as cheap peptides. Price tells you almost nothing about what’s actually in the vial.
Are these things even legal, and how worried should I be about safety?
Depends heavily on where you are and how you get it. In the US, most SARMs sit in a legal grey zone, unapproved for human use. Some peptides need an actual prescription if you’re getting them pharmaceutically. On safety: SARMs carry documented testosterone-suppression and liver risks. Peptides look cleaner in early data but lack long-term human trials, so treat both with real caution, not just the SARMs.
Written by Fatima Delgado, independent journalist. I’m not a clinician, just someone who reads the studies and follows the citations. Last reviewed February 2026.
For background only. Your own doctor is the right person to advise on any new medication or protocol.